In another section of this website, we have discussed how an anesthesiologist work is broken into start-up units, time units and modifiers to create a unit total. This is then multiplied by a unit value to get a total to charge a payer. This installment will give a rudimentary discussion about how groups share their collections.
Why is this important?
Anesthesiologists work at sites where work is brought in by others with the expectation that service will be provided without regard to insurance or payment. Similarly, call requirements may require a physician to be on site for long periods of time, and yet may not result in payment. When unit support is provided, there needs to be a mechanism to divide it. As you might expect, with the wide variety of combinations of hospitals, surgery centers and physician’s offices, every group comes up with their own solution. As you consider accepting a position with a group, you will want to understand their formula.
Eat What You Bill
When physicians are working alone, this is the most basic level of reimbursement. Units are totaled, and bills are sent. Collections arrive, and what is paid becomes your income. Thirty years ago, it wasn’t uncommon for groups of anesthesiologists to be all solo with little collaboration. This was possible because the variation between governmental and private payers was small and there was little unit support paid by hospitals. Today this is more commonly seen in surgery centers with a few rooms and dedicated anesthesiologists. Success relies on the shared interest of bringing in payers with good reimbursement and controlling hours of operation.
Salary
A salary model is attractive because you know up front how much money you will make. It can work well when you have a good understanding of the expectations that accompany the salary. What is the call burden and frequency? How many hours per week are expected? What happens if workload changes? (Illness, injury, leave for other group members.) Can you increase your income? And if so, how?
For many groups using a salary model there is a quarterly bonus that is used to distribute additional collections. Be sure to ask how this money is apportioned. It is important to remember that whenever someone is paying a salary, there has been a calculation to make sure that there is enough money to cover expenses when collections are 15% less than expected. If there is extra, does it go to the doctors or to someone else?
Unit-Based Distribution- ASA Units
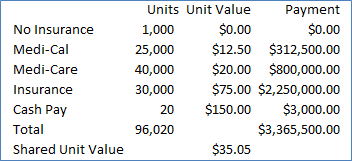
Many groups pool collections, then share them based on workload. The numerator they use for distribution is ASA units, or some modified variation thereof. To remove the risk that any member gets disproportionately affected with poor payment patients, the group blends all cases to come up with a shared unit value.
In the example to the right, we see a simplified calculation for determining a shared unit value. Total units billed are calculated over a time period, and divided into total calculations to determine a “Shared Unit Value.” Anesthesiologists’ income is determined by multiplying their individual units by the Shared Unit Value to determine their income.
Limitations of this method include: 1) short cases with high unit values (Endo, Cataracts, PE Tubes) can lead to inflated incomes, 2) past payer mixes may not remain the same in the future. For this reason, most practices will have methods to compensate to make sure they don’t run into cash flow issues.
Unit-Based Distribution- Hours Worked
Some groups use hours worked as their work unit. This puts the focus on working collaboratively to get the work finished, rather than keeping individual units. It can align a hospital or surgery center’s priorities with the anesthesiologists’ priorities.
Stipends For Call And Specialty Care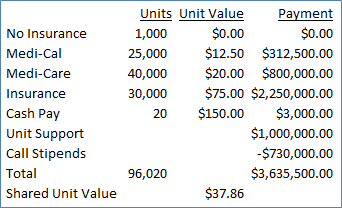
Hospital based groups usually carve out a segment of their income for duties that may not generate income. Money has now been added in to assist with providing stipends for call coverage as well as augmenting the Shared Unit Value.
Groups can use the same methodology to carve out extra money for Cardiac, Regional, Pediatric, Leadership duties, or any other item deemed worthy of support outside the unit value system.
Other Considerations
Unlike restaurants, anesthesiologists are not paid at the time of service. In the best of circumstances, the process of data input, coding, and transmission of claims takes at least a week, and the portion of collections from insurers takes at least a month. The patient portion, (which continues to grow) can stretch out for months, if it ever arrives. How do groups adapt to this?
Most practices build in a look-back to allocate monies to doctors that reflect the work that is done in a time period. The mechanism is to pay out a safe portion of collections, and leave an accumulation to make adjustments that reflect actual rather than predicted. Some try to make the calculation precise, while others are content to make a good faith effort to recognize and compensate for the work / income irregularities.
Summary
Anesthesiologists’ income can be derived in multiple ways. The above examples can be used in isolation or can be blended together (i.e., Salary for the first 8 hours, units for work after 1500). When looking at a practice, ask someone to describe the process used to determine how monies coming into the practice are distributed to the doctors. I would recommend focusing more on their understanding how things are shared, rather than the minutia.